
Remember me

Survival outcomes in this ‘STAMPEDE-like’ cohort provide some insights into the management of high-risk prostate cancer in the PSMA-PET era. Higher sensitivity and specificity of PSMA-PETCT for index staging in high-risk prostate cancer, coupled with dose-escalated, hypofractionated radiotherapy to prostate and nodes, can achieve high disease control with LT-ADT alone. The MFS and PCSS in our cohort are similar to the test arm of STAMPEDE, without systemic intensification.
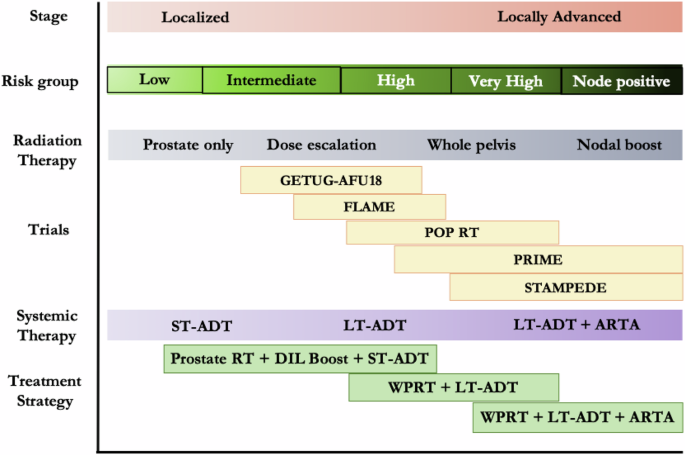
Across the spectrum of high-risk prostate cancer, various strategies for local and systemic treatment intensification have been used (Fig. 1). ‘Augmented radiotherapy’ by escalating dose to the whole prostate or the dominant lesion, and nodal irradiation may be adequate for early high-risk disease. Dose escalation to 80 Gy in the RTOG 0126 randomised trial improved DMFS with only modest increase in late toxicity [7]. Similarly, pelvic radiotherapy showed 6.7% higher 5-year MFS with no significant increase in late morbidity [6, 8]. While a 6-year MFS of about 80% in our cohort using local intensification is encouraging, it may be further improved by systemic intensification. Patients with worse prognosis due to multiple high-risk factors or nodal involvement may be preferentially selected for addition of ARTA to radical radiotherapy and LT-ADT [9].
Fig. 1: Prostate cancer risk spectrum and treatment intensification strategies.
ADT androgen deprivation therapy, ST short term, LT long term, RT radiotherapy, WPRT whole pelvic radiotherapy, ARTA androgen receptor targeted agents.
The benefit of abiraterone must be put in context of its adverse effects profile and cost. In the STAMPEDE trial, 37% of men reported severe adverse events with abiraterone and 13% needed to discontinue the drug. Additionally, regulatory and financial barriers limit access to abiraterone globally, including many high-income countries [10]. An elaborate quality-adjusted life years based analysis by the STAMPEDE investigators suggests that addition of abiraterone to ADT would be cost-effective for non-metastatic prostate cancer if it costs less than 28 GBP/day [11]. Ongoing randomised trials are exploring alternative ARTAs including enzalutamide (ENZARAD, NCT02446444), apalutamide (ATLAS, NCT02531516; NRG GU-009 PREDICT-RT), and darolutamide (THUNDER, NCT06282588; DASL-HiCAP-ANZUP1801, NCT04136353), or using novel imaging (PRIME, NCT03561961; THUNDER) and genetic biomarkers (THUNDER, NRG GU-009 PREDICT-RT), refining systemic therapy for high-risk prostate cancer.
Although we have made all attempts to check the veracity of the data, we acknowledge the inherent limitations of survival outcomes from a retrospective study in a limited single-institution cohort. Additionally, the PSMA-based MFS as used in this cohort is different from the CI-based MFS used in the STAMPEDE trial. The events for PSMA-MFS occur earlier but may not correlate with OS, though using CI at recurrence in our cohort would have resulted in a higher MFS than reported.
Treatment intensification, be it local or systemic, comes at a cost and should be done judiciously. Addition of ARTA to augmented radiotherapy and LT-ADT may benefit patients with node-positive disease, multiple high-risk factors, or in the absence of PSMA-PET imaging. PSMA-PET imaging exemplifies the potential of advanced diagnostic tools to refine treatment. However, it also needs a nuanced understanding of phenomena like the Will Rogers effect to interpret clinical outcomes accurately and ensure optimal patient care. The ongoing trials will provide more answers for personalising treatment for high-risk prostate cancer.
Comments (0)