
Remember me


Atypical hemolytic uremic syndrome (aHUS) is a rare, potentially life-threatening condition; however, the evidence currently guiding therapeutic strategies remains inconsistent across countries.
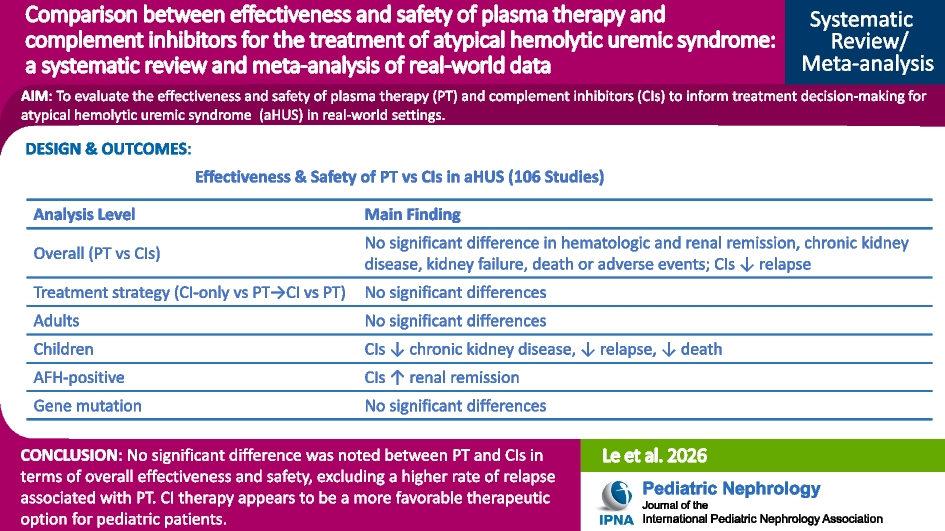
ObjectivesIn this meta-analysis, we evaluated the effectiveness and safety of key therapeutic strategies, including plasma therapy (PT) and complement inhibitors (CIs), with the goal of informing treatment decision-making for aHUS in real-world settings.
Data sourcesPubMed, Embase, and the Cochrane Library were searched, without date or language restrictions.
Study eligibility criteriaObservational cohort studies examining the effectiveness and safety of PT and CIs in patients with aHUS were included.
Study appraisal and synthesis methodsStudy quality was assessed using the Newcastle–Ottawa Scale. Target outcomes included initial treatment responsiveness (hematologic and renal remission) as well as progression and prognosis, including chronic kidney disease (CKD), kidney failure, relapse, death, and adverse events.
ResultsData were obtained from 106 observational cohort studies. No significant difference was observed between PT and CIs in terms of overall effectiveness or safety, with the exception of a lower relapse rate for CIs (0% vs. 15.5%, p < 0.001). Subgroup analysis revealed no significant differences between patients receiving CIs as first-line therapy, switching from PT to CIs, or receiving PT alone. In adults, no significant difference was observed between PT and CIs in terms of initial treatment response, prognosis, or safety. However, in children, CI therapy was associated with lower rates of CKD (24.6% vs. 56.6%, p < 0.001), relapse (6.2% vs. 25.5%, p = 0.02), and mortality (0.3% vs. 7.6%, p = 0.002) compared with PT. In patients with positive anti–complement factor H antibodies, CI therapy was associated with a higher rate of renal remission compared with PT (90% vs. 41.8%, p = 0.02), with no significant differences observed in any other outcomes. In patients with complement gene mutations, no significant differences in outcomes were observed between CIs and PT.
Conclusions and implications of key findingsNo significant difference was noted between PT and CIs in terms of overall effectiveness and safety, excluding a higher rate of relapse associated with PT. CI therapy appears to be a more favorable therapeutic option for pediatric patients.
Prospero registrationCRD420251239582.
Graphical Abstract
Comments (0)