Notably, this proof-of-concept study assessed the safety, feasibility, and survival outcomes of conversion therapy in patients with initially unresectable stage III NSCLC specifically. The treatment was well tolerated with manageable postoperative morbidity and satisfactory efficacy. The biomarker for responders of ICT was also revealed.
It has been controversial whether surgery could serve as a therapeutic modality for initially unresectable stage III NSCLC after downstaging with induction treatment. Durvalumab after definitive concurrent chemoradiotherapy is the standard treatment for the unresectable stage III NSCLC, which demonstrates favorable efficacy in PACIFIC study, with a 12-month progression-free survival (PFS) rate of 55.9%.18 Thus, the conversion surgery after induction therapy should be verified to be with a similar efficacy without drawing the unacceptable surgical-related complications.
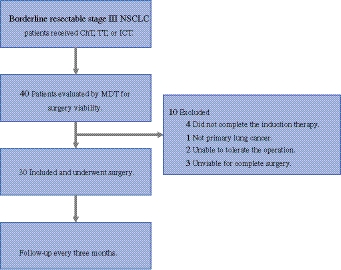
The rates of morbidity were 13.0–40.0% in three prospective trials of neoadjuvant therapy for potentially resectable stage IIIA to IIIB NSCLC, and 13.0–16.1% in two retrospective trials of induction therapy for initially unresectable stage IIIB NSCLC.7,8,10,11,19 Further, 3 out of 24 patients (12.5%) who underwent surgery after induction therapy encountered surgical-related complications in a latest published exploratory study for unresectable stage II–III NSCLC.9 Our study demonstrated a postoperative morbidity rate of 33.3% and 30–90-day mortality rate of 3.3%, which were similar to abovementioned data, thus acceptable.
In terms of induction therapy, our regimen presented with optimistic nodal downstaging rate (26/30, 96.2%), MPR rate (20/30, 66.7%), and pCR rate (8/30, 26.7%). These short-term outcomes affirmed the efficacy of this treatment strategy.
It is widely acknowledged that the long-term prognosis of patients, including EFS and OS, is the most important criterion for evaluating the effectiveness of a cancer treatment regimen. At 12 months, the rate of EFS was 87.5%, and OS was 96.7%, which were even better than the result of PACIFIC, illustrating its potential benefit on survival.
The finding above highlighted and advanced the position of radical surgery in the treatment strategy of initially unresectable stage III NSCLC.
In addition, regimens of induction therapy in our study were ICT, ChT, and TT. Among them, ICT was the most common therapy in our study and also in other trials, exhibiting a favorable rate of MPR (16/22, 72.7%) and pCR (6/22, 27.3%). The MPR/pCR rate was 100% (4/4)/75% (3/4) in TT group and 33.3% (1/4)/0.0% (0/4) in ChT group. Unfortunately, further comparison was unavailable due to the great difference of sample size in the three groups, which could be the topic for future discoveries.
Regarding potential biomarkers for responders of ICT, we identified a B cell immune-related gene set, which may serve as a promising predictor for the MPR and OS. It is commonly believed that cytotoxic T cells are the directors of antitumor immunity in tumor microenvironment (TME), which made them the core of most tumor immunology research. Notably, the tumor-infiltrating B lymphocytes (TIBs) are also essential members of tumor-infiltrating lymphocytes (TILs), which carry strong prognostic significance.20 B cell regulates tumor-driven antibody-mediated immune responses through mechanisms of complement dependent cytotoxicity (CDC), antibody-dependent cell mediated phagocytosis (ADCP), and antibody-dependent cell mediated cytotoxicity (ADCC). Previous results have shown that B cell infiltration in NSCLC was significantly higher than that in nontumoral tissue.21 Follicular B cells, plasma cells, and germinal center (GC) B cells were the main subsets of TIBs in NSCLC with their own gene signatures, of which the plasma cells were identified to be predictor of OS in patients treated with atezolizumab, but not chemotherapy.22 The components of our B cell immune-related gene set were all included in the three B cell subsets signatures identified in the aforementioned analysis. We believe this is the first study to verify enrichment of B cell immune-related pathways in MPR post-treatment NSCLC samples, which proves the close relationship between B cell immunity and therapeutic response. Additionally, the gene set we produced has strong potential to be the predictor of survival for patients who received immunotherapy.
This study has several limitations. Firstly, it adopts a single-arm study design, lacking data from a control group undergoing durvalumab after definitive concurrent chemoradiotherapy. Secondly, the participants received three different patterns of induction therapy, which increased the heterogeneity. Third, invasive mediastinal staging was performed in only a subset of patients at baseline, whereas post-induction nodal status was confirmed by pathological assessment of systematically dissected lymph nodes at surgery. Therefore, nodal downstaging, defined by comparing baseline nodal staging with postoperative pathological nodal status, should be interpreted with caution, particularly in patients whose baseline nodal status was determined radiographically. Another limitation is that this study was entirely based on the single-center population, thus limiting the generalizability of the results. In addition, the relevance between the B cell immune-related gene set and B cell antitumor immunity in TME should be verified in future research. These gaps lay the groundwork for further investigation in future research.

Comments (0)