In 2004, Busam et al. classified DM into “pure” and “combined” subtypes, the latter now more commonly referred to as “mixed” DM.7 While pDM is characterized by fusiform melanocytes with ≥ 90% stromal fibrosis, mDM has less (10–90%) stromal fibrosis with areas of densely packed tumor cells. These subtypes have been reported to differ in biological behavior, with mDM demonstrating higher rates of lymph node involvement in previous studies.5,8
In our meta-analysis, the pooled SLN positivity rate was 6% among patients with pure DM and 15% among those with mixed DM—a threefold difference. When all studies were pooled without distinction between subtypes, the overall SLN positivity rate was 9%, a value likely reflecting the combined inclusion of both pure and mixed lesions. The absence of an association between SLN positivity and traditional prognostic features such as Breslow depth or ulceration further suggests that nodal spread in DM may be influenced more by histologic subtype than by conventional clinicopathologic factors. These findings support the selective use of SLNB in patients with mixed DM, aligning with current practice for other cutaneous melanomas. SLNB provides pathologic staging and prognostic information but does not inherently confer clinical benefit. Although randomized trial data in conventional cutaneous melanoma support potential outcome benefit for SLNB in selected patients with intermediate-thickness disease,27,28 comparable evidence demonstrating clinical benefit in desmoplastic melanoma is lacking.
Distinguishing between histologic subtypes is also critical for interpreting the existing literature on SLN outcomes in desmoplastic melanoma. In prior studies, reported rates of SLN positivity have ranged widely: from 0 to 18.2% in pDM, and from 0 to 33.3% in mDM,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26 likely reflecting small samples sizes and inconsistency in subtype classification. Although the majority of included studies applied the 2004 Busam et al. classification system to differentiate between pDM and mDM, 3 of the 10 studies did not.16,19,24 For example, one study inferred pDM classification from the absence of mixed features noted in the pathology report.24 Variability in diagnostic rigor, as well as differences in anatomic site distribution, may further explain the heterogeneity across cohorts. Standardized histopathologic definitions and consistent reporting of subtype are therefore essential for accurate risk assessment and future guideline development.
Large, pooled databases were not included in our study due to the possibility of overlapping patient populations with several of the institutional cohorts included in this meta-analysis. Several SEER-based analyses have reported markedly lower SLNB positivity rates in desmoplastic melanoma compared with institutional series. In one multicenter study that compared prospective trial data with SEER (1998–2009), the SEER cohort demonstrated an SLN positivity rate of only 2.5% (15/594), far below the 17% rate observed in their combined institutional dataset.20 SEER analyses focused specifically on head and neck desmoplastic melanoma have yielded similarly low estimates, with reported SLN positivity rates of 3.7% in a cohort of 244 patients and 5% in a cohort of 165 patients undergoing SLNB.29,30 These lower rates likely reflect the inherent limitations of large population-based registries, including heterogeneity in patient selection for SLNB, lack of standardized diagnostic criteria distinguishing pure from mixed desmoplastic melanoma, and variability in the rigor of pathologic examination across reporting institutions. Such differences underscore the need for caution when interpreting SEER-derived estimates in the context of SLNB decision-making for desmoplastic melanoma.
The role of traditional clinicopathologic predictors such as Breslow depth and ulceration in desmoplastic melanoma remains controversial and appears to differ from that in other cutaneous melanomas, particularly once histologic subtype is established. While Breslow thickness and ulceration are well-established predictors of sentinel lymph node positivity in conventional melanoma,20,26,31,32,33 multiple studies have demonstrated that pDM frequently presents with greater tumor thickness yet exhibits substantially lower rates of nodal metastasis compared with mDM and nondesmoplastic melanomas.14,21,24 This paradoxical pattern suggests that histologic subtype may function as a dominant modifier of nodal metastatic risk in desmoplastic melanoma, potentially limiting the predictive value of conventional risk factors for SLNB decision-making. Prior studies evaluating Breslow depth and ulceration in desmoplastic melanoma have yielded mixed results and have often focused on survival outcomes rather than SLN positivity.20,24 As such, the incremental value of these traditional predictors for SLNB selection in subtype-defined desmoplastic melanoma remains uncertain and is unlikely to be fully resolved without large scale individual patient-level analyses.
The associations between SLN positivity and Breslow depth and ulceration status were assessed for the full cohort using study-level meta-regression, as both factors are independently associated with SLN positivity in cutaneous melanoma.31 Given the use of aggregate rather than individual patient-level data, these analyses should be interpreted as exploratory. Subtype-specific meta-regression was not feasible owing to inconsistent reporting of Breslow depth and ulceration within pure and mixed cohorts across studies. In contrast to conventional melanoma, we found no significant association between SLN positivity and either Breslow depth (\(\beta\) = 0.058, p = 0.749) or ulceration status (\(\beta\) = 0.763, p = 0.677) for patients with DM. Egger et al. found that ulceration status, but not Breslow depth, was associated with a positive SLNB in patients with DM and that SLN positivity and ulceration were independent predictors of worse disease-free survival.20 The discrepancy between these findings likely reflects the limited power and interpretability of study-level analyses in a rare disease, as well as the overall low incidence of nodal metastasis in desmoplastic melanoma and the inclusion of mixed cohorts in which pure and mixed subtypes were not uniformly distinguished. These factors, together with inconsistent reporting of tumor-level characteristics such as Clark level, microsatellites, and mitotic rate, substantially limit the ability of pooled analyses to define reliable clinicopathologic predictors of SLN involvement in this rare melanoma subtype.
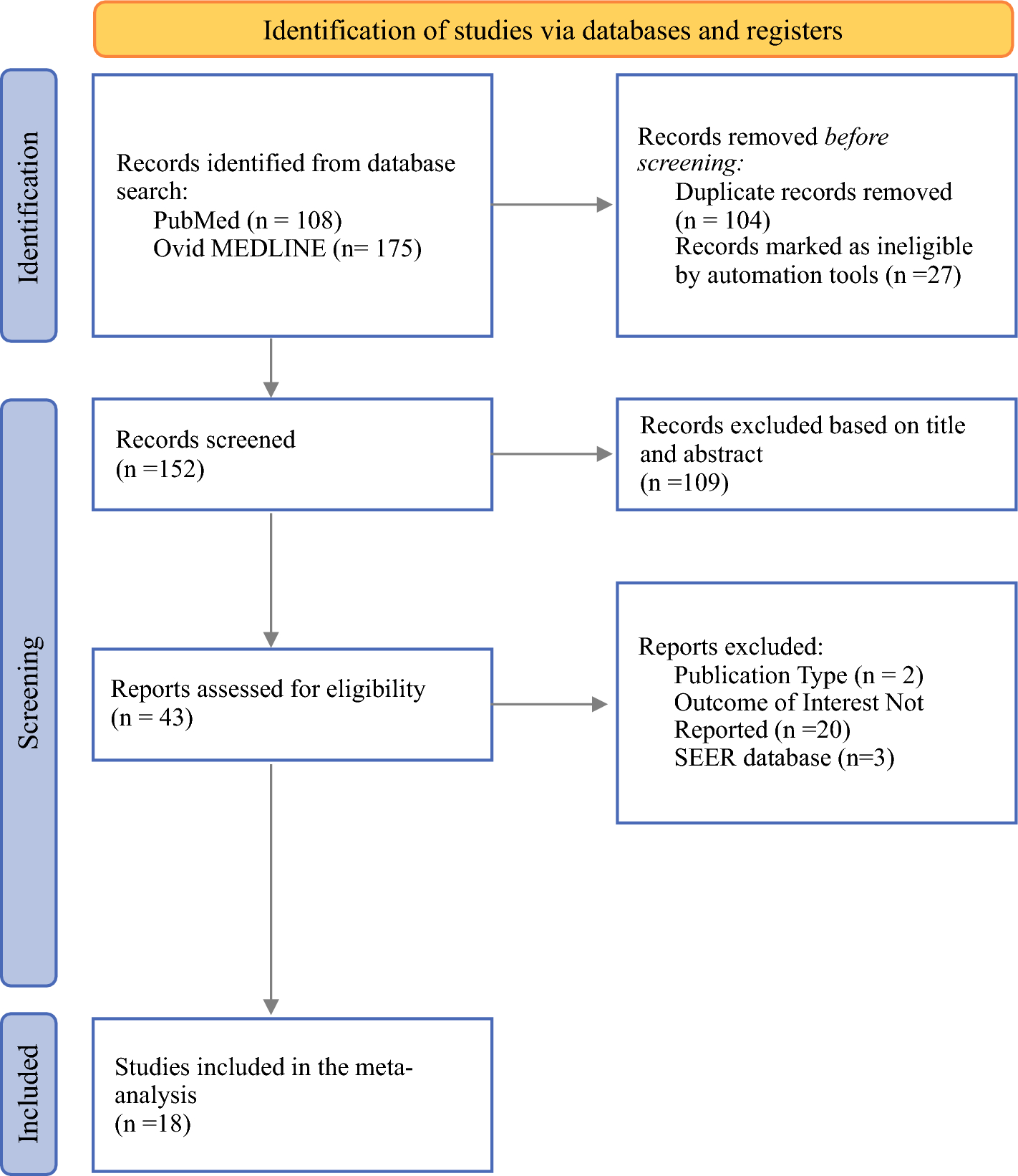
The overall methodological quality of the included studies was moderate-to-high based on the Joanna Briggs Institute critical appraisal. Most studies clearly defined inclusion criteria, reported consecutive patient inclusion, and provided adequate follow-up. However, the analysis is limited by the predominance of small, retrospective case series and the absence of patient-level data in many reports, which restricted stratified analyses and reduced the power of meta-regression. Inconsistent histopathologic criteria for diagnosing desmoplastic melanoma and subclassifying pure versus mixed subtypes also contributed to variability across studies. Visual inspection of the funnel plot did not suggest publication bias, and the pooled analyses demonstrated low statistical heterogeneity; however, in the context of rare-event meta-analyses, I2 values near zero should be interpreted cautiously, as limited event rates may reduce the power to detect true between-study heterogeneity. Despite these limitations, our study is strengthened by its systematic methodology, adherence to PRISMA guidelines, and use of random-effects modeling with subgroup and meta-regression analyses, providing clinically relevant pooled estimates to inform sentinel lymph node biopsy decision-making in patients with desmoplastic melanoma.

Comments (0)