Emissary veins emerge during fetal development as auxiliary outflow channels when the rapidly enlarging transverse sinuses outpace the capacity of the sigmoid sinus and IJV, and a variable number persist postnatally with highly diverse morphologies [12]. The extracranial fenestration documented here most likely reflects incomplete coalescence of parallel plexiform venous channels during this developmental process, representing part of the recognised spectrum of extraaxial developmental venous anomalies [10].
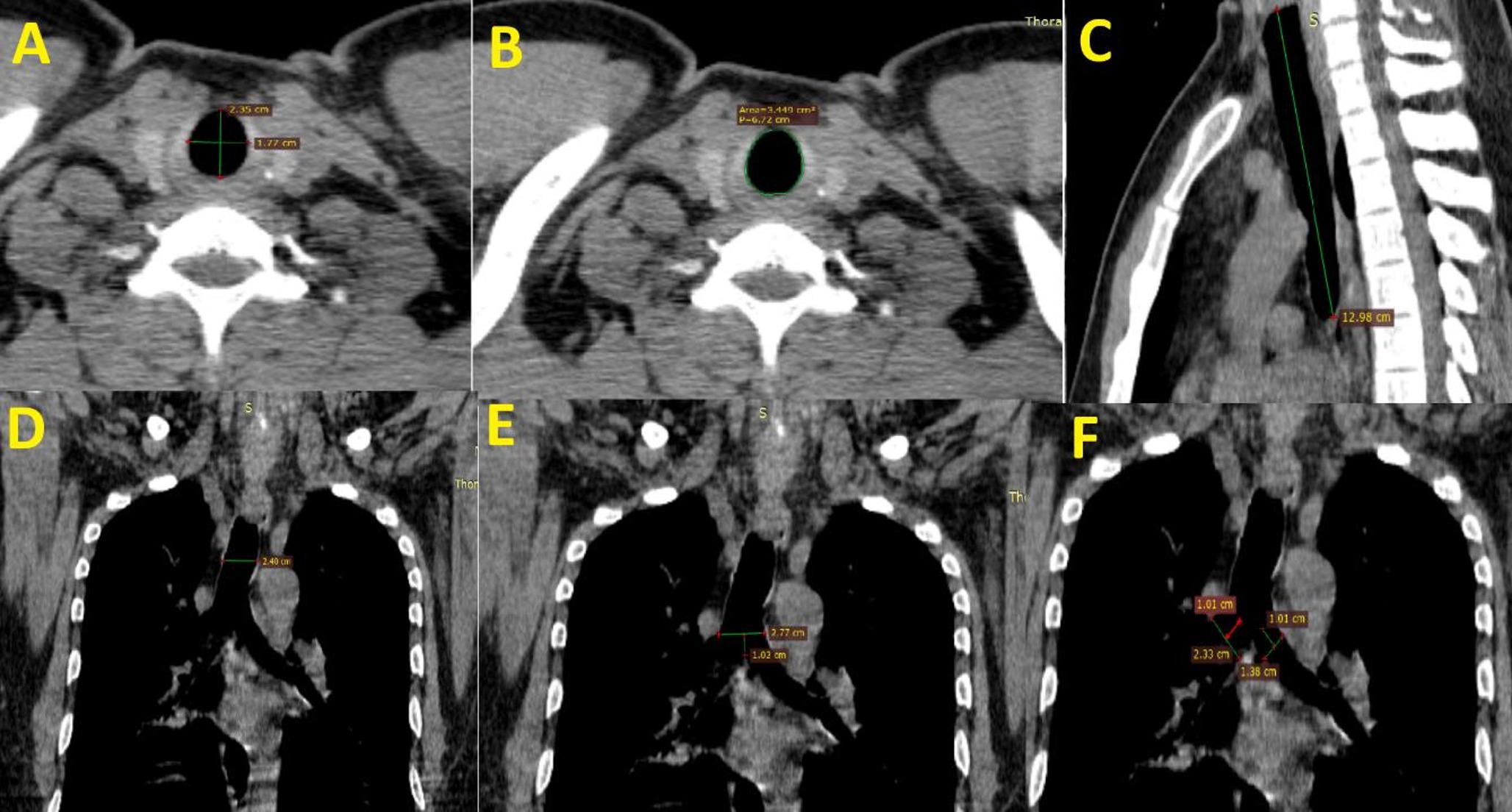
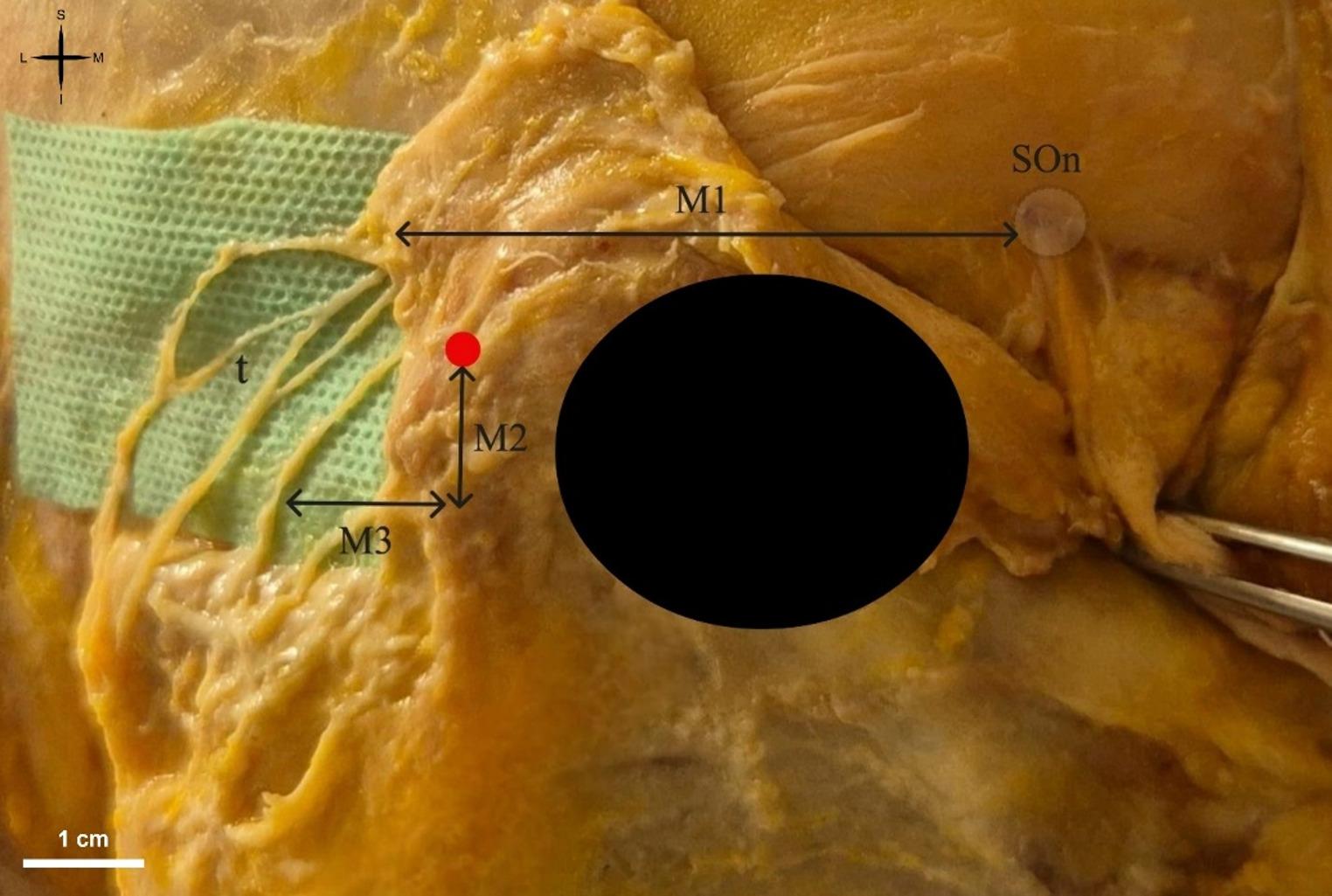
The present case demonstrated a large MEV (6.6 mm) exiting a single mastoid foramen and forming a 2.33 cm-long extracranial fenestration shortly distal to the foramen, with three deep communicating veins to the suboccipital venous plexus and distal continuation as the deep cervical vein.
From a morphometric perspective, the diameter observed here is well above the typical ranges reported in imaging and dry skull series. There were reported mastoid emissary foramen diameters up to 5.0 mm on the right and 4.4 mm on the left in an MDCT cohort [5]. D’Mello et al. (2025) summarised that most MEVs in published series are < 2–3 mm, with enlarged veins (> 4–5 mm) forming a small minority [3]. Our 6.6 mm MEV exceeds the 3.5 mm threshold proposed as clinically significant and falls within the range that has been associated with operative bleeding in modern otologic series [3, 13].
Multiplicity of the bony pathway, multiple mastoid emissary canals/foramina or accessory canals, has been described in anatomical and imaging studies, including high-resolution CT and cone-beam CT [5, 6, 11, 13, 14]. In our case, however, the bony exit was single, and the variation occurred extracranially as a split-and-rejoin segment (fenestration). Such a configuration could be misinterpreted as two independent veins on non-contrast imaging and may be relevant if the MEV is evaluated as a surgical corridor landmark or as a target for occlusion.
The three anastomoses with the suboccipital venous plexus and the continuation as the deep cervical vein support the concept that the MEV can participate in posterior neck venous drainage pathways. Emissary veins may assume a major collateral outflow function when normal jugular outflow is altered [13], and the multiple extracranial communications in our case could represent a robust collateral route. The MEV was recently highlighted as one of the named tributaries of the condylar emissary venous plexus in the occipitoatlantal region, further underscoring its role in the suboccipital venous communication network and its potential to contribute to uncontrolled intraoperative bleeding during upper cervical procedures [16].
Unilateral vertebral artery hypoplasia is not an uncommon finding, with a pooled prevalence of 13.41% reported in a recent meta-analysis of 176,391 subjects across 32 studies encompassing the V3 and V4 segments [15], and prevalences as high as 40.9% recorded in large MRI series when a broader diameter threshold is applied [2]. The calibre reduction of the left V4 in our case is therefore consistent with a recognised anatomical variant rather than acquired stenosis, further contextualised by the fact that a transdural origin of the PICA, itself a facultative content of the VA dural ring, was identified in 5.56% of vertebral arteries in a dedicated CTA prevalence study [4].
Venous pulsatile tinnitus due to enlarged MEV has been documented as unilateral or bilateral and has been managed successfully by surgical ligation or endovascular coiling/embolization in selected patients [1, 8, 9, 17]. Although the present case was identified during anatomical documentation rather than in a symptomatic setting, a fenestrated segment may be clinically relevant if occlusion is planned, because persistent flow through an unoccluded limb could theoretically maintain symptoms or promote collateralisation.
From a surgical perspective, the mastoid and suboccipital regions are frequently traversed in posterior fossa surgery and are increasingly traversed in otologic implant procedures. High-resolution CT has been recommended for identifying mastoid emissary anatomy preoperatively [6, 13], and D’Mello et al. (2025) emphasised a review of prior temporal bone CT to mitigate avoidable bleeding risk during Osia implantation [3]. Our findings extend this message by showing that clinically relevant variation may occur beyond the bony canal, emphasising careful evaluation of the extracranial venous segment when contrast-enhanced imaging is available.
Limitations of this report include its single-case design and the lack of haemodynamic or clinical correlation. Nevertheless, recognition of extracranial fenestration as a possible MEV variant adds nuance to radiological interpretation and may assist surgeons and interventionalists working in the posterior mastoid and upper cervical region.


Comments (0)