
Remember me

This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Life and Health Sciences Research Institute – ICVS (reference number: CEICVS 171/2023). The procedure was developed and validated in the anatomy laboratory using fresh-frozen cadaveric specimen donated for research and educational purposes. Donors had provided informed consent prior to death, and specimens were handled in compliance with institutional and ethical standards. Each specimen was thawed at room temperature for 24 h before dissection.
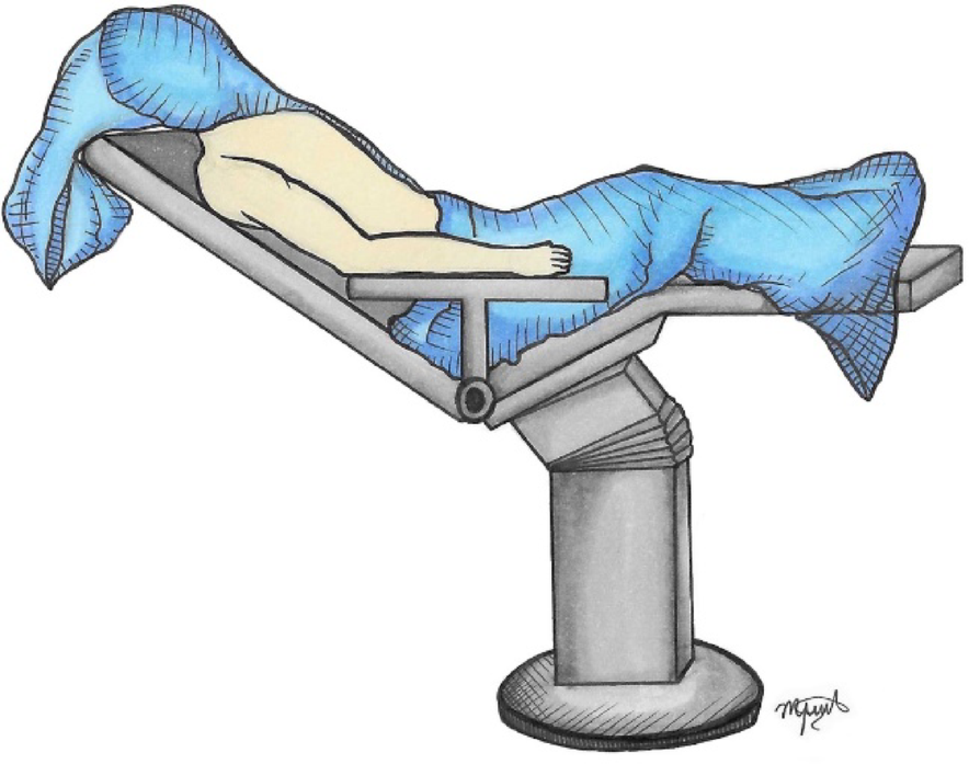
Patient setupThe patient is placed in the beach-chair position with the affected arm resting neutrally at the side, optionally supported by a mechanical arm holder (Fig. 1). Before incision, the ACJ is reassessed under fluoroscopy for reducibility, and anatomical landmarks (clavicle, acromion, and coracoid) are carefully marked.
Fig. 1
Patient positioning and surface anatomy. Beach-chair position with neutral arm support. Anatomical landmarks (clavicle, acromion, coracoid) marked prior to incision
ApproachIn addition, a 3 cm mini-open incision is made over the ACJ to allow debridement, facilitate joint reduction, and expose the deltotrapezial fascia and ACJ capsule.
ReductionThe ACJ is anatomically reduced, and it can be temporarily stabilized with two Kirschner wires after aligning their articular facets [4] (Fig. 2). Reduction is confirmed under fluoroscopic control.
Fig. 2
AC joint reduction. A 3-cm mini-open incision over the AC joint allow exposure and debridement. The joint is reduced anatomically and stabilized provisionally with Kirschner wires, confirmed under fluoroscopy
Harvest of the LHBTThe LHBT is released approximately 1 cm proximal to the musculotendinous junction. A subpectoral tenodesis is performed with a suture anchor, preserving elbow flexion and forearm supination strength, while maximizing graft length for reconstruction.
Arthroscopic stepsPortals and Rotator Interval and Coracoid Exposure.
Three standard arthroscopic portals are created: posterior, anterolateral, and anteromedial. The rotator interval is opened to visualize the coracoid base. The subcoracoid space is cleared, ensuring adequate visualization and working area (Fig. 3).
Fig. 3
Surgical approach. Three arthroscopic portals allow the endoscopic-assisted procedure with inspection of the joint, secure the LHB tendon and opening of the rotator interval to visualize the coracoid base
The proximal stump of the LHBT is redirected proximally, maintaining its native supraglenoid attachment. The tendon is delivered through the anteromedial portal, prepared extracorporeally with Krackow stitches on the free end using high-strength number two sutures, and the diameter is measured (typically 4–5 mm in diameter). The graft is trimmed and calibrated so that its diameter does not exceed 4.0 mm, ensuring compatibility with the clavicular tunnel.
Coracoclavicular tunnel (elastic system passage)A 2.4 mm guidewire is advanced from the superior clavicle, approximately 4.5 cm medial to the ACJ, toward the base of the coracoid under arthroscopic and fluoroscopic control. A drill guide system (Conmed Infinity ACL/PCL Femoral Footprint Guide Arm, Infinity Guide Body, Infinity Guide Sleeve Straight 2.4 mm – Conmed, Largo, FL, USA) is used at an angulation of 70–80°. A 2.0 mm hole is created after fluoroscopic confirmation, the suspensory fixation system (Infinity Button – Conmed, Largo, FL, USA) is passed and secured, using a suture passer (Super Shuttle – Conmed, Largo, FL, USA) to shuttle both suture strands, thereby restoring vertical stability.
Clavicular Tunnel for the LHBT graftA second tunnel is then prepared for the tendon itself, drilled in the clavicle more laterally than the suspensory system. This tunnel is placed around 3 cm medial to the ACJ and drilled to 4.0 mm diameter to allow passage of the LHBT graft. The prepared tendon is introduced with the aid of a suture shuttle, maintaining continuity with its native origin at the supraglenoid tubercle.
Acromioclavicular cerclage and graft fixationOnce the graft is retrieved above the clavicle, it is tensioned and cycled. An additional set of sutures placed 2–2.5 cm from the tendon extremity is passed through a horizontal 2.0 mm tunnel in the clavicle (2 cm medial to the ACJ) and then through a horizontal/oblique tunnel in the acromion (2 cm lateral to the ACJ). These sutures create a cerclage construct across the ACJ, reinforcing horizontal stability. The residual posterosuperior capsule and AC ligament are sutured and plicated to the graft to augment resistance and stability (Fig. 4).
Fig. 4
Coracoclavicular tunnel for suspensory fixation, AC cerclage and graft fixation. A 2.0 mm tunnel (VC2) is drilled from the clavicle to the coracoid base at 4.5 cm medial to the AC joint. The suspensory fixation system (Infinity Button) is passed with a Super Shuttle device to shuttle both suture strands, restoring vertical stability. A second tunnel (VC1) drilled 3–3.5 cm medial to the AC joint with a diameter of 4.0 mm, accommodates the calibrated LHBT graft. The graft is tensioned and cycled. Sutures from its free end are passed through a 2.0 mm clavicular tunnel (HC1) and a horizontal/oblique acromial tunnel (HA1), creating a cerclage that reinforces horizontal stability. The residual posterosuperior capsule and AC ligament are sutured and plicated to the graft to augment construct stability. HA1 – Horizontal Acromium 1; HC1 – Horizontal clavicle 1; VC1 – Vertical clavicle 1; VC2 - Vertical clavicle 2
Verification and closureFinal joint stability is confirmed arthroscopically and fluoroscopically. Portals and the ACJ mini-open incision are closed in layers, and sterile dressings are applied.
Anatomical evaluationThe primary outcome was the feasibility and reproducibility of the technique under endoscopic assistance. Secondary outcomes included anatomical accuracy of graft passage, correct positioning of fixation points, and absence of neurovascular conflict.
So, following completion of the procedure, specimen was carefully dissected to verify graft trajectory, tunnel positioning, and the relationship of the graft to adjacent neurovascular and capsuloligamentous structures to confirm reproducibility and anatomical safety. The key Pearls and Pitfalls of the technique are summarized in Table 1.
Table 1 Pearls and pitfalls of using the long head of the biceps (LHB) tendon as a pedicular autograft in AC joint reconstruction
Comments (0)