
Remember me
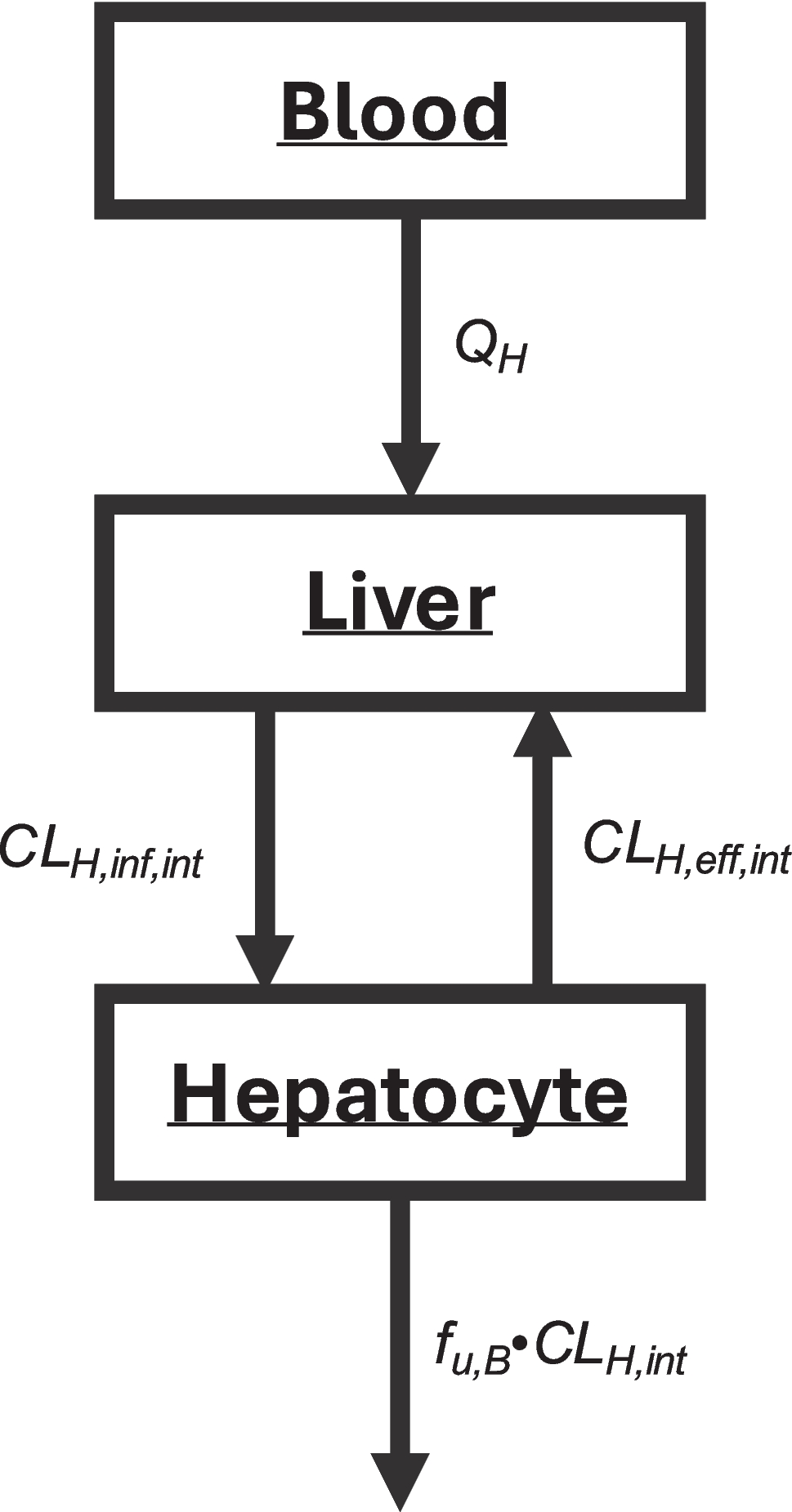

A minimal PBPK model structure, implemented within the Simcyp Simulator V22 (Certara Predictive Technologies, Certara UK Ltd, Sheffield, UK) was used to develop the model for bevacizumab. Multiple publications supported using this model structure to capture the disposition of mAbs (16, 17, 20). The minimal PBPK model incorporated a tissue compartment subdivided into vascular, endosomal, interstitial, and intracellular spaces, a central lymph node and a central plasma compartment. The dynamic movement of the TP is simulated by blood flows into and out of the tissue, along with the lymphatic flow (21). The PK data for bevacizumab used in the model were collected across multiple clinical trials and previously utilized in bevacizumab popPK analyses (6, 7). Because bevacizumab PK shows dose proportionality with dose levels ranging from 1 to 20 mg/kg (4), target-mediated drug disposition (TMDD) was not considered in the PBPK modeling, as the doses investigated in the clinical trial included in the analysis were within the dose proportional range. Figure 1 provides an overview of the overall modeling strategy.
Fig. 1
Development, verification, and application of a minimal PBPK model for bevacizumab in adult and pediatric populations
Bevacizumab PBPK Model Development in AdultsThe model parameters for bevacizumab includes the molecular weight, binding affinity to FcRn at pH 6, and the clearance of bevacizumab (Table I). The distribution between the vascular and interstitial space through the fluid-filled pores by convection and diffusion is calculated by two-pore hypothesis, which considers the hydrodynamic radius (Rs) and size of the tissue pores. The vascular reflection coefficient through large and small leaky pores (σv,l and σv,s) and permeability surface area product for large and small pores (PSs and PSl) in the tissue pores are calculated from physiological and drug-specific parameters (22). Bevacizumab is also uptaken into endothelial cells through fluid-phase endocytosis, when binding with FcRn, the drug is protected from catabolic degradation and is recycled (17, 23). The endosomal uptake (Kup), recycling (Krc), and catabolic clearance (CLcat) parameters are evaluated for exogenous IgG and are assumed to be the same for IgG1-like antibody bevacizumab (21). Binding affinity to FcRn (KD1) was fitted to plasma concentration–time profiles for adults to be 0.884 uM (18).
Table I Final Parameters Value for Bevacizumab PBPK ModelThe initial performance of the PBPK model was assessed through simulations with 100 virtual 70-kg adult patients receiving different intravenous (IV) bevacizumab dose regimens (15 mg/kg every three weeks, 10 mg/kg every two weeks, and 5 mg/kg every two weeks). PBPK-simulated exposure metrics (the geometric mean of AUC0-tau, Cmax, and Cmin) for Cycle 1 and steady state were compared with popPK model-simulated exposure metrics. The popPK model simulations were performed based on 70-kg adult patients, with males exhibiting a higher clearance and volume of distribution compared to females (6). The popPK simulation was implemented using NONMEM version 7.5. In the final PBPK model, an additional clearance parameter (CLadd) was included to account for other elimination pathways with unknown mechanisms. This parameter was optimized based on the popPK model-simulated AUC0-tau, Cmax, and Cmin at steady state for IV bevacizumab 15 mg/kg every three weeks, 10 mg/kg every two weeks, and 5 mg/kg every two weeks.
Bevacizumab Model Verification in Adult PatientsTo verify the model in adults, bevacizumab PK data from clinical studies was used to assess the model performance. The verification process leveraged individual data from clinical studies to ensure the robustness of the PBPK model. From the 786 adult patients, 7,750 PK samples were included in the analysis (Table S1), providing a rich dataset with various bevacizumab doses to capture the demographic variability among patients (6). This large pool of samples allowed for a detailed analysis of the bevacizumab concentration–time profile. Out of the initial cohort of 786 adult patients, 605 patients were selected for model verification based on the following criteria to ensure that the dataset was representative of the patient population of interest: the patients receiving IV bevacizumab dose of 15 mg/kg dosed every three weeks, 10 mg/kg dosed every two weeks, and 5 mg/kg dosed every two weeks. Additionally, the patients in the verification set included those with breast cancer, non-small cell lung cancer, metastatic colorectal cancer, and pancreatic cancer, which provided a diverse tumor types.
PBPK model simulations were performed using 100 virtual adult patients aged 18 years and above. This approach enabled an exploration of bevacizumab PK using a virtual population, ensuring the model could predict PK profiles for a broad range of patient characteristics. The patient characteristics of age, height, and weight were summarized in Table S2 by dose level.
The simulations included both single and multiple dosing of bevacizumab. This aspect of the model verification was crucial as it mirrored the various dosing schedules used in clinical practice, thereby testing the model’s ability to predict bevacizumab PK across different dosing scenarios. By comparing the simulated PK profiles with the observed clinical data, the model performance to predict bevacizumab concentrations was assessed. Specifically, PBPK model-simulated PK profiles were overlaid with observed PK data after single dose administration (Cycle 1), stratified by sex and by dose level (15 mg/kg, 10 mg/kg, and 5 mg/kg). The age range and the average height and weight based on observed data were fixed for the 100 virtual adult patients in each single dosing simulation scenario.
However, for multiple dosing (Steady State), observed PK from all patients could not be summarized together, due to inconsistent adherence to the dosing regimen. Instead, 18 patients who had PK samples collection at steady state concentrations were randomly selected and their PK data were compared individually. The exposure metrics (AUC0-tau, Cmax, Cmin) at Cycle 1 and steady state were also compared between observed and model-simulated values. For multiple dosing, one out of 18 patients was selected at a time with 100 virtual adult patients simulation performed, and the simulation mimicked the actual data from the patient in terms of age, height, weight, dose, and time of administration.
Bevacizumab PBPK Model Development in Pediatric PatientsIn the model, both maternal and pediatric IgG contributions were combined to reflect the physiological changes. Following birth, the maternal IgG concentration declines in the first three months of life and de novo synthesis of IgG in pediatrics gradually increases. The overall endogenous IgG level reaches 50% of the adult level by the end of the first year of life and adult levels at around 10 years (16). FcRn abundance was assumed to be consistent between pediatric and adult populations (17). Lymph flow data for pediatrics have not been quantified. Therefore, lymph flow in adults was scaled allometrically using an exponent of 0.75 for pediatric subjects, leading to a total lymph flow that was 2.6 times higher in neonates compared to adults (16). The proportion of total lymph flow contributed by each organ or tissue was assumed to be consistent between children and adults (24). An ontogeny scaling factor was integrated into the additional clearance parameter to facilitate the extrapolation of the model to the pediatric population (ages 0.5 to18 years). The ontogeny scaling factor incorporates Simcyp’s age, weight, and height equations, with the clearance scaled with an allometric exponent of 0.75 based on body weight from the popPK analysis for males and females. This scaling factor is used to calculate the additional clearance fraction from birth to 18 years olds, and the age effect is illustrated in Figure S1.
Bevacizumab Model Verification in Pediatric PatientsTo verify the PBPK adult model in data from pediatric patients, bevacizumab PK data from 141 pediatric patients and 1,423 PK samples across five Phase I to IV clinical trials were utilized (7). The large number of patients and samples allowed for detailed characterization of bevacizumab PK profile in pediatric patients (6 months to 18 years), capturing the variability in drug disposition across different age groups and tumor types. The patient cohort included individuals with various cancers such as solid tumors, gliomas, osteosarcoma, rhabdomyosarcoma, and non-rhabdomyosarcoma soft tissue sarcoma. This diverse patient population ensured that the model was verified across a wide range of clinical conditions, providing a robust dataset for model assessment.
Pediatric PBPK simulations were conducted for each pediatric patient in the clinical trials using 100 virtual pediatric patients. The demographic and physiological characteristics of each set of 100 virtual pediatric patients reflected the observed characteristics of each patient in the clinical study. The simulations for multiple dosing regimens of bevacizumab mimicked the actual dosing level and administration time that the pediatric patients received. The model’s predictions were compared with the observed PK data from the clinical trials. In addition, the following number of patients were selected for each age bin for detailed comparisons: 6 patients between 6 months and 2 years, 15 patients between 2 and 6 years, and 12 patients between 12 and 18 years. For further assessment of the pediatric PBPK model performance, simulations results from the younger age range of 6 months to 12 years were compared with the outputs from the popPK model simulations.
Sensitivity AnalysisGlobal sensitivity analyses were conducted to investigate the parameter with the highest impact (i.e. recycling rate, endosomal uptake rate via fluid-phase endocytosis, and FcRn abundance) on the plasma concentration profile and exposure metric (AUC) of bevacizumab, while keeping other model parameters constant. The evaluated ranges for uptake rate (Kup), recycling rate (Krc), and FcRn abundance were 0.000298–2.98 h−1, 0.0313–313 h−1, and 0.086–8,600 μM, respectively. In the virtual pediatric population, the analysis focused on the variability in the endogenous IgG and FcRn abundance. The evaluated ranges for FcRn abundance and endogenous IgG were 0.086–8600 µM and 1200–16500 µg/mL, respectively.
Comments (0)