
Remember me

The DSC analysis revealed that the melting point of aripiprazole was approximately 81 ̊ C, consistent with values reported in the literature (Supplemental Fig. 1) (20). This suggests that the vehicle used in the preparation of Aristada® does not influence the melting behavior of the API. The DSC thermogram displayed a single sharp endothermic peak corresponding to crystalline aripiprazole, with no additional peaks observed. This indicates that aripiprazole lauroxil does not form hydrates or solvates in the dispersion medium. TGA was performed to quantify residual organic solvent in aripiprazole lauroxil API, as excessive residual solvent could affect solubility and, consequently, dissolution behavior. The residual solvent content was found to be approximately 0.254%, which is considered low (Supplemental Fig. 1) (21).
Solubility AnalysisSolubility analysis was conducted to evaluate the solubility of aripiprazole lauroxil in various media, as it is a critical parameter in formulation development. It did not exhibit a significant solubilized fraction across different pH conditions, which may be attributed to its extremely low aqueous solubility. In the commercial suspending medium, only a small amount (~ 7 µg/mL) of aripiprazole lauroxil was in the solubilized form, which is negligible compared to the administered dose of 441 mg/1.6 mL. This low solubility suggests a minimal potential for initial burst release in vivo for Aristada®. The small solubilized fraction may be due to the presence of excipients such as Tween 80 and polyethylene glycol (PEG) in the dispersion medium. Additionally, solubility studies were performed using varying concentrations of surfactants in water to assess potential release media. Both Tween 80 and sodium dodecyl sulfate (SDS) demonstrated a concentration-dependent increase in solubility (Supplemental Table 1).
PXRD AnalysisThe PXRD pattern of the dried drug product (Aristada®) exhibited distinct sharp peaks, indicating a crystalline nature. The most intense diffraction peak was observed at 2θ ~ 4.9 (Supplemental Fig. 2), suggesting the presence of a highly ordered crystal lattice. Additional characteristic peaks were observed at approximately 10.9 ̊, 15.2 ̊, 17.8 ̊, 18.9 ̊, 20 ̊, 21.5 ̊, 23.4 ̊, and 25.8 ̊ (2θ). No significant amorphous halo was detected, indicating the absence of an amorphous phase in the sample analyzed.
Particle Size AnalysisParticle size is a critical formulation attribute for LAI suspensions, as variations during manufacturing process can significantly impact product performance (22, 23). The mean particle size of Aristada®, measured using the MasterSizer™, Malvern Instruments, UK, was approximately 28 µm with a calculated SPAN value of 1.38. The cumulative Dv10, Dv50 and Dv90 were 13.87 µm ± 0.88, 28.74 µm ± 0.96, 53.54 µm ± 0.71, respectively (n = 3).
Additionally, microscopy imaging under polarized light revealed that the particles exhibited birefringence, indicating the crystalline nature of aripiprazole lauroxil. The dispersed particles were irregular in shape and lacked defined geometry, which could be attributed to the milling process used during formulation or heterogeneity arising during crystallization. Moreover, some particles appeared to be aggregated, possibly due to hydrophobic interactions (Supplemental Fig. 3).
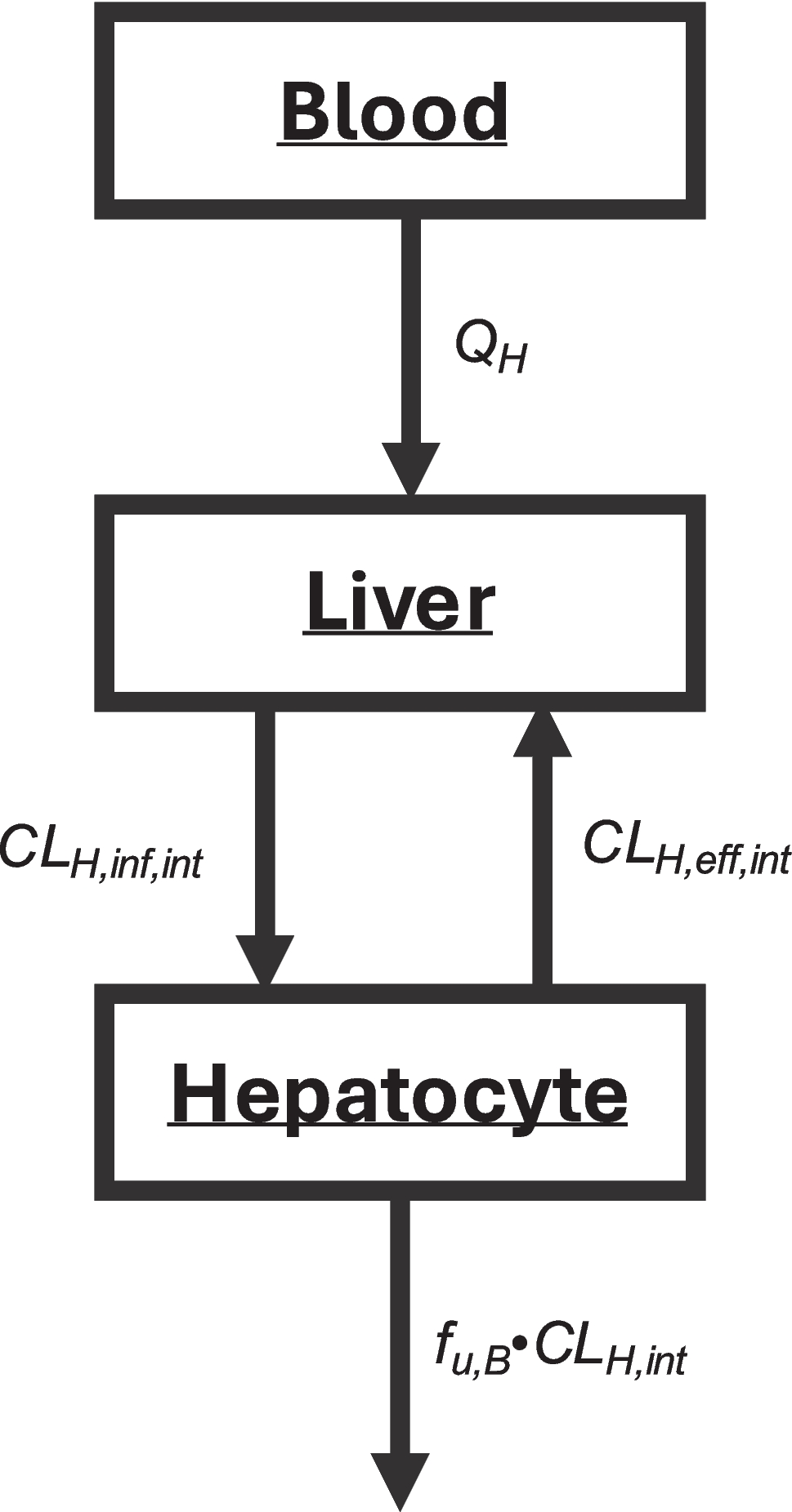
Systemic ModelAR plasma concentration data following IV (2 mg) infusion, and oral solution (15, 20 and 30 mg) administration were best described by a three-compartment model. Across the investigated dose range (2 to 30 mg), AR demonstrated a linear systemic PK with a linear hepatic clearance (CLH) of 0.03028 L/h/kg; volume of central, second and third compartments of 1.5825L/kg, 2.0831L/kg and 9.1754 L/kg, respectively and constants k12: 0.22832 h−1, k21: 0.17345 h−1, k13: 0.01108 h−1, k31: 0.001911 h−1. For clinical scenarios used for model development, the simulated/observed ratio ranged from 0.88 to 1.23 for Cmax and from 0.92 to 1.05 for AUC0-t, as shown in Fig. 2 and Table III. The 20 mg and 30 mg solution doses were mispredicted during the absorption phase (first few hours) after dosing, however the distribution/elimination phases were well predicted. Slight absorption misprediction is not impactful for the subsequent use of the model since intestinal absorption is not relevant to the intramuscular model.
Fig. 2
Observed (symbols) and predicted (solid lines) AR plasma concentration vs time profile after intravenous infusion (2 mg) and oral solution (15, 20 and 30 mg) administration of aripiprazole in humans. Dataset used for model development (Table I)
Table III. Comparison of Cmax and AUC0-t fold-errors after AR IV and oral administrationData from several other clinical scenarios were used to externally validate the model: oral solution (5 and 10 mg) and oral tablet (5, 10, 15, 30 mg) administrations. The simulated/observed ratio ranged from 0.87 to 1.18 for Cmax and from 0.88 to 1.04 for AUC0-t, as shown in Fig. 3 and Table III. Hence, the developed model adequately described the observed plasma profiles of AR following oral administration in humans with all the simulated Cmax and AUC0-t values within ± 25% of the observed values (Table III). Based on the simulation results, the systemic distribution and elimination model was deemed acceptable to be used for IM simulations.
Fig. 3
Observed (symbols) and predicted (solid lines) AR plasma concentration vs time profile after oral solution (5, and 10 mg) and oral tablet (5, 10, 15 and 30 mg) administration of aripiprazole in humans. Dataset used for model external validation (Table I)
Intramuscular ModelThe calculated IM Kp and fut for AR were 1.84 and 0.12%, respectively. These parameters were used to simulate AR systemic exposure following its IM solution administration in healthy humans (12). The simulated AUC0-t for IM administration of AR solution was within 25% of the observed value (observed: 1423.2 ng-h/ml; predicted: 1645.3 ng-h/ml; fold-error: 1.16). The fold error on Cmax was more significant (observed: 20.6 ng/mL; predicted: 28.7 ng/mL; fold-error: 1.39), but within the considerable observed variability (Fig. 4). A possible explanation for the high variability from solution injection may be missed injection site (24), as the IM solution was dosed into the gluteus maximus, i.e. some of the dose could have been dosed to adipose tissue (reported BMI range 18–30 kg/m2, mean BMI: 25.5 kg/m2) (12). To test this hypothesis, the IM Kp and fut were adjusted to the median value between the calculated muscle and adipose, i.e. Kps 1.84 and 9.84, respectively, median Kp = 5.84, and futs 1.20E-03 and 2.24E-04, respectively, median fut = 0.712E-03. This resulted in better prediction for Cmax (predicted: 22.1 ng/mL; fold-error: 1.07). The reported average of individual Cmax and Tmax were 23.7 ng/mL (CV% 41) and 3 h (range 0.50 h −10 h), respectively. The predictions with both Kps and futs were within the range of observed values for Cmax and Tmax, which supports the hypothesis of missed injection site.
Fig. 4
Observed (symbols) and predicted (solid lines) AR plasma concentration vs time profile after IM administration of aripiprazole solution in healthy humans
Given the variability in the observed data during the absorption phase, and the uncertainty as to how much could have been dosed into the subcutaneous space, the approach of calculating IM Kp with the default methods was maintained and the IM Kp for AR was kept at the calculated value of 1.84. The IM absorption model approach, i.e. Kp and fut default calculation methods, were deemed acceptable to be used for the AR-L IM suspension simulations. Additionally, upon administration of a poorly soluble compound like AR, precipitation can happen at the injection site, which was not accounted for in the model.
The systemic AR PK model was used to simulate AR exposure after IM administration of Aristada (AR-L suspension) at three dose levels (150, 300, and 400 mg AR equivalent). AR-L is synthesized with a proprietary technology (LinkeRx; Alkermes) designed to create a pro-drug from molecules that lack a hydroxyl functional group, such as AR. The modified properties of the pro-drug (AR-L), such as low solubility, result in extended systemic release after injection (10, 19). Such compounds can be formulated as simple aqueous suspensions, and dissolution of AR-L is the rate limiting step in the depot followed by rapid absorption of the pro-drug into systemic circulation (19).
The calculated IM Kp and fut for AR-L were 4.28 and 2.25E-06%, respectively. The initial prediction was based on the assumption that the absorption rate is solely dependent on the dissolution of AR-L and partitioning of the dissolved AR-L into the systemic circulation from the IM depot. The simulation results showed a shape mismatch between the simulated curve and observed data and an earlier predicted Tmax (Fig. 5). The predicted exposure (AUC0-t) was in better agreement with the observed values, indicating a discrepancy in the transfer rate and further model adjustments were needed. I.e., predicted Cmax and AUC0-t for the 150, 300 and 400 mg doses were Cmax 44.8 ng/mL and AUC0-t 48,270 ng-h/mL; Cmax 115.11 ng/mL and AUC0-t 123,600 ng-h/mL; Cmax 153.48 ng/mL and AUC0-t 164,700 ng-h/mL, respectively.
Fig. 5
Observed (symbols) and predicted (lines) AR plasma concentration vs time profile after IM administration of aripiprazole lauroxil (AR-L) suspension in humans. Comparison of model with and without the inclusion of Immune cell layer. Left axis: plasma concentration (ng/mL); right axis: ICL thickness (µm)
The delayed appearance in systemic circulation after IM administration of AR-L suspension may be attributed to the formation of a dynamic ICL around the injected material (depot). The ICL presents an additional barrier for the dissolved drug to diffuse through before reaching the systemic circulation, explaining the delayed Tmax.
The calculated drug diffusivity and fraction unbound of AR-L in the ICL, and the ICL surface area were 1.12E-6 cm2/s, 0.34245% and 2.32 cm2, respectively (Eqs. 2, 3 and 4). The ICL parameters A and B (Eq. 1) were 2.09E-6 cm/hr and 0.012 1/hr respectively, which were fitted to the observed PK data for the 400 mg equivalent IM Aristada dose. The same ICL thickness kinetic was used to simulate the other IM Aristada doses. The inclusion of an ICL in the model resulted in adequate predictions (fold errors less than 25%) of the exposure parameters (Table IV) and of the shape of the plasma concentration–time profiles (Fig. 5) for all three dose levels.
Table IV. Comparison of Cmax, AUC0-t and Tmax fold-errors after AR-L IM administrationParameter Sensitivity AnalysisThe model without ICL was only sensitive to solubility, particle size and diffusion layer thickness (Supplemental Fig. 4). Even though the model was sensitive to these parameters, varying them was not sufficient to capture the observed data. The only way to properly describe the observed data was through the inclusion of ICL.
The impact of lag time (i.e., time elapsed before the onset of ICL) is demonstrated in Fig. 6a. In the absence of ICL, the drug can dissolve and be absorbed unimpeded, resulting in rapid uptake into systemic circulation during the hours that ICL was not present. Lower values of ICL-A parameter will reduce the thickness of the ICL whereas higher values increase the ICL maximum thickness. The impact of ICL-A parameter is shown in Fig. 6b. The impact of ICL-B parameter, which, together with ICL-A, modifies the length of time that the ICL takes to reach maximum thickness, is shown in Fig. 6c. The particle size impact is shown in Fig. 6d. Only after the ICL decay did the particle size play a role, i.e. while ICL was in place (first 300 h) the impact of particle size was minimal, however, after the ICL decay, the smaller the particle size, the higher the exposure.
Fig. 6
Parameter Sensitivity Analysis on ICL parameters Lag Time (a), magnitude (b), rate (c) and particle size (d). Baseline values for each variable: Lag Time = 0 h; Magnitude = 2.09E-06; Rate = 1.2E-02 and Particle Size = 14.18 µm
Comments (0)